
 Contact
Contact Hours
Hours Location
Location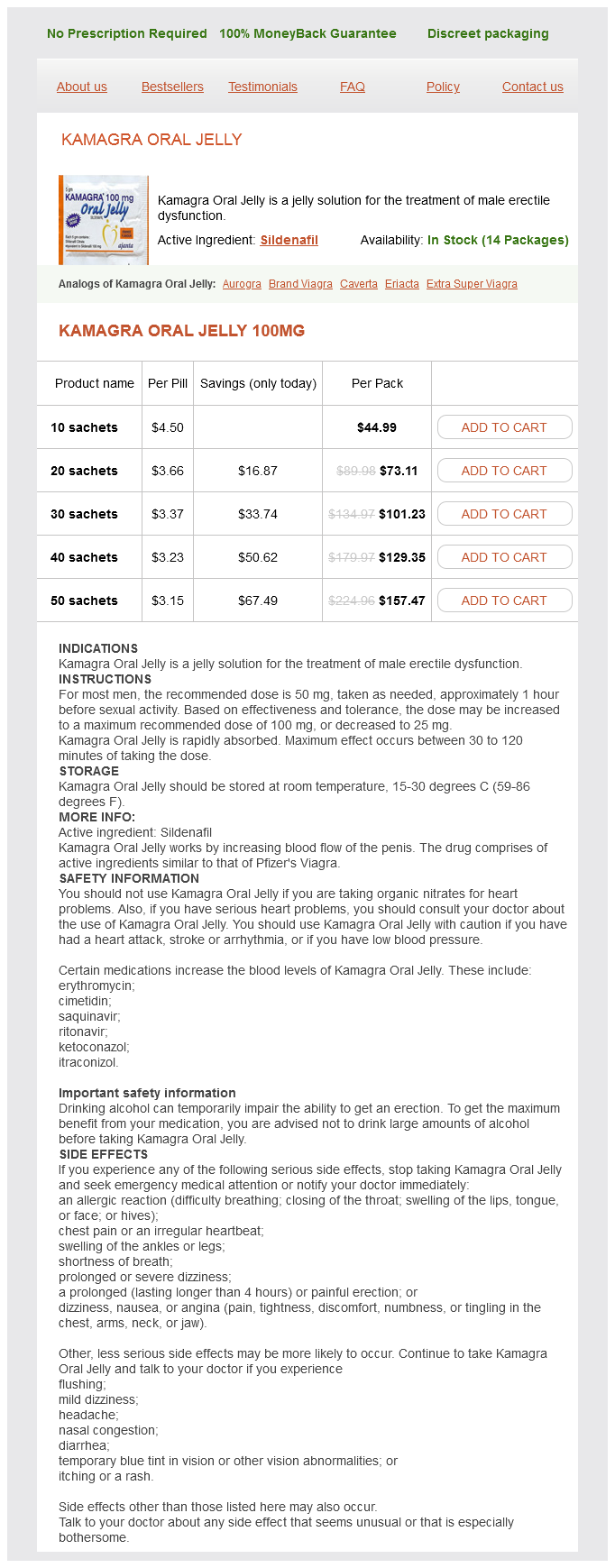
Kamagra Oral Jelly dosages: 100 mg
Kamagra Oral Jelly packs: 10 sachets, 20 sachets, 30 sachets, 40 sachets, 50 sachets
Only $3.35 per item
In stock: 826
Description
Fiberoptic lighting may assist in viewing the extent of radial styloid involvement erectile dysfunction pills supplements kamagra oral jelly 100 mg purchase free shipping. The argon beam coagulator may be used to achieve hemostasis in the cavity and may have a beneficial effect as an adjuvant causing surface necrosis. A dorsal approach maximizes exposure and facilitates subsequent intercalary arthrodesis. Mobilize the flexor tendons, median nerve, and ulnar nerve away from the tumor-bearing segment. Alternatively, the midcarpal articulation can be excised en bloc with the tumor-bearing segment by cutting with an oscillating saw from dorsal to palmar through the distal aspect of the distal carpal row bones. Dorsal exposure of the distal radius and ulna with transection of the radius and ulna prox- imally. The resection specimen, demonstrating the midcarpal articulation of the proximal carpal row. Reconstruction is by means of an osteoseptocutaneous vascularized fibula graft for intercalary arthrodesis. Activities are gradually in~eased, with high-risk activities being restricted for up to 2 years due to cryon~osis of bone caused by cryosurgery. Formal supervised therapy is initiated at the first dressing change, typically 8 to 10 days after surgery. Protective splinting continues a total of 6 weeks minimum after intralesional procedures and until bone healing is confirmed after arthrodesis. The local recurrence rate after curettage, cryosurgery, and cementation of distal radius giant cell tumor of bone is about 20% to 25% and corrdates with soft tissue extension. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement. CctmpliC4ted syndactyly refers to the interposition of accessory phalanges or abnormal bones between digits. The true incidence of syndactyly is wlk:nown, in part be· cause of the difficulty distinguishing mild simple syndactylies from normal web spaces. Simple incomplete syndactylies of the bilateral third web spaces, with the left hand more severely affected. Simple complete syndactyly of the second and third web spaces is seen in another patient. Local skin £laps should be used to r&:reate the couunissure to avoid scar contracture and "web creep. Judicious defatting of the skin flaps should be perfonned to facilitate skin closure, reduce tension across the flaps, and improve the aesthetics of the reconstructed fingers. Positioning · the patient is positioned supine with the affected limb sup· ported on a hand table. Approach · the principles of separation for simple complete syndactyly are weD accepmJ; however, there is tremendous variation in the surgical incisions and skin flap designs used for these operations. Dorsal skin flaps are preferred for commissure reconstruction, because of their pliability and ability to recreate the normal dorsal-proximal to volar-distal slope of the web.
Syndromes
- Dry eyes
- Disseminated intravascular coagulation (DIC) -- a clotting disorder that leads to excess bleeding (hemorrhage)
- Gender
- Pre-diabetes: 5.7% to 6.4%
- HIV infection
- Located over the site of a wound or injury
The individual recovering from the injury attempts to return as much as possible to a level of maximum engagement and productivity in the community causes of erectile dysfunction in your 20s purchase kamagra oral jelly 100 mg online, while the family settles into longer-term patterns and equilibrium that allow them to resume their family life cycle with an altered identity. This is when discouragement, depression, despair, and mourning begin to occur, often over the first few years after the end of rehabilitation. The crucial turning point occurs when, after all formal rehabilitation ends, the family as a system faces the challenge of being able to reconstitute as an effective and functional system with a new balance and identity. In families who cannot, the life cycle is seriously disrupted, and individual members may be blocked from making natural life transitions in a healthy way. For example, a busy professional couple may be unable to reorganize their time and finances to care for a severely injured son who lives at home, and that role may fall to a teenage daughter. If she becomes trapped in that role, she may stay home after high school and devote herself to caring for her brother, with the result that her own development (college, career, boyfriends, marriage) may be seriously blocked. Depending on her nature, she may either become seriously depressed or sacrifice herself for the sake of the family to her longterm "detriment. The decision to intervene when the selfsacrifice is in the service of homeostasis raises difficult countertransference and ethical issues, which must be dealt with honestly both by the therapist and directly with the family. Even when families do make the transition and their life cycle resumes, transitional points can bring episodic issues. Families that were dysfunctional before the injury may require formal family therapy after the injury, with the added complication of learning to adjust their family structure. This broad division, however, is useful in conceptualizing the nature of interventions that must be made during each stage. In the acute stage, in which the primary issues are survival, medical stabilization, and minimization of permanent damage, the family generally coalesces, suspends normal routines, and orients all of its energy toward the care of the injured person. This is a period of crisis intervention when education and information are crucial. Emotional support and permission to break standard family routines also are important. Later within this stage, when survival is assured, the family must quickly evaluate treatment options and insurance realities. Family intervention should be aimed at helping the family to cope effectively on numerous fronts while still in shock, including practical daily realities, emotional distress, and major decision making. The rehabilitation stage is defined as the intermediate stage during which formal restorative treatment, inpatient or outpatient, is the primary family focus. This is a time when high expectations for recovery predominate, and the family begins the task of receiving the injured person back into the family system and making the necessary structural adjustments. Family roles are reorganized, and the goal is the restoration of as much physical and cognitive functioning as possible after brain injury. During this stage, there is initially relief at survival and great hope for recovery, which the therapist should support, while gradually tempering hope with cautious reality. Even when therapists realistically assess severe limits of long-term functioning, families may be angered and alienated if this message is presented prematurely or too starkly. It is much better to help families gradually realize (rather than be told) emerging limitations through experience.
Specifications/Details
Hexacosanol (Policosanol). Kamagra Oral Jelly.
- What is Policosanol?
- Are there any interactions with medications?
- Are there safety concerns?
- Dosing considerations for Policosanol.
- How does Policosanol work?
- High cholesterol, inherited high cholesterol (familial hypercholesterolemia), intermittent claudication, increasing blood flow to the heart in people with coronary heart disease, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96177
Individuals with versional oculomotor deficits primarily report reading difficulties: reading slowly erectile dysfunction treatment hong kong order kamagra oral jelly 100 mg, loss of place while reading, misreading or rereading words and paragraphs, text that appears to "swim" and "shimmer," and, occasionally, apparent visual motion perhaps related to vergence misalignment and/or frank oscillopsia. Some of these symptoms may also be related to vestibular deficits (see the section Visual-Vestibular Disturbances later in this chapter, as well as Chapter 22, Dizziness, Imbalance, and Vestibular Dysfunction). Oculomotor rehabilitation is also beneficial for versional deficits (Ciuffreda et al. Vision-related symptoms associated with near-work include eyestrain (ocular "fatigue"), intermittent closing of one eye, diplopia, abnormal sensitivity to visual motion, and the perception that printed text is "floating above the page" or "shimmering. Vertical Oculomotor Deviations Vertical oculomotor deviations, including heterophorias and heterotropias, are more complex to manage because of the variability in magnitude of the deviation as a function of gaze position and time of day. If oculomotor rehabilitation is unsuccessful, and surgery is not an option, then occlusion of one eye as needed to eliminate diplopia may be recommended. Although neurological or mechanical restriction of the extraocular muscles does limit the benefit of oculomotor rehabilitation for increasing the range of horizontal and vertical fusion, it still should be attempted to improve vision function and overall visual efficiency (Han et al. Patients with visual-vestibular disturbances report difficulty shopping in department stores with high shelving because of the sensation of visual motion in their periphery (Bronstein 2004), being in visually crowded environments such as busy restaurants, watching movies or television because of the rapid movement from scene to scene, reading because of the sensation of "shimmering" and "floating," and using the computer monitor because of screen flickering. Patients with vestibularly based symptoms are referred typically to neurology, neurotology, and, finally, vestibular rehabilitation, an area in which vision becomes especially important (Bronstein 2004; Bucci et al. Despite the fact that the patient and target are stationary during standard clinical binocular vision testing, unstable fusion in association with symptoms of nausea and dizziness during the actual binocular vision clinical testing is often evident in patients with vestibular dysfunction. Oculomotor rehabilitation, with the incorporation of fusional prisms for diplopia and tinted lenses for photosensitivity, is designed to improve and stabilize fusional vergence under static and dynamic viewing conditions at all distances and directions (Ciuffreda 2002). Additionally, as stated in the section Refractive Changes, it is important to prescribe single-vision spectacles for patients requiring different corrections for far and near viewing for presbyopia and accommodative deficits. Recent research suggests that there are two major categories of photosensitivity: 1) increased sensitivity to all types of lighting, and 2) increased sensitivity predominantly toward fluorescent lighting. Although the neurological correlates for generalized or fluorescent photosensitivity have not yet been elucidated, the discomfort associated with both categories of photosensitivity may be alleviated considerably by wearing brimmed caps and using tinted lenses, with a lighter tint used for indoors and a darker tint used outdoors (Jackowski 2001; Kapoor and Ciuffreda 2002). Patients with hemianopia report either of the following: 1) "being told" that part of their visual field is missing, if they have visual inattention; or 2) being aware that part of their visual field is missing, if they do not have visual inattention. Hemianopic patients may also report that they bump into objects on one side, miss food on one side of the plate, have trouble dressing one side of their body, and have problems navigating streets and buildings (Hellerstein 1997; Hellerstein et al. It often limits their independence through the restriction or even prevention of common tasks, such as driving and unaccompanied ambulation. Scanning techniques, either alone or in conjunction with a field-enhancing optical device (Suter 2007), may also benefit the patient (Kapoor et al. Patients presenting with this type of field loss typically do not report functional vision limitations. Curr Treat Options Neurol 4:271280, 2002 Suh M, Basu S, Kolster R, et al: Increased oculomotor deficits during target blanking as an indicator of mild traumatic brain injury.
Related Products
Additional information:
Usage: q.i.d.
Tags: cheap kamagra oral jelly 100 mg amex, kamagra oral jelly 100 mg buy on-line, kamagra oral jelly 100 mg low cost, order kamagra oral jelly 100 mg on-line
8 of 10
Votes: 270 votes
Total customer reviews: 270
Testimonials
Sivert, 42 years: It may be deemed necessary by my doctor that I see a medication-use specialist at any time while I am receiving controlled substance medications. Penile and clitoral erection are influenced by sensory innervation through the pudendal nerve, proerectile parasympathetic innervation, antierectile sympathetic innervation, and somatic innervation that contributes to penile rigidity. Initial literature on this entity cited a 24% incidence of labyrinthine concussion in patients with closed head trauma (Griffiths 1979). This vascular anatomy supports the concept that peripheral injuries can heal if injured and treated appropriately, whereas tears of the central portion do not heal if sutured and are usually dtbrided.
Vak, 38 years: Arch Phys Med Rehabil 89:1887 1892, 2008 Paniak C, MacDonald J, Toller-Lobe G, et al: A preliminary normative profile of mild traumatic brain injury diagnostic criteria. Use an aseptic non-touch technique to ensure that only sterile items come into contact with the susceptible site that sterile items do not come into contact with nonsterile objects and that key parts are not touched. The study found that depression was the most significant factor associated with aggression, and that depression was also associated with other traumatic complaints, younger age at injury, and low life satisfaction (Baguley et al. Observations of patient participation by clinical staff also have been used to index motivation (al Adawi et al.