
 Contact
Contact Hours
Hours Location
Location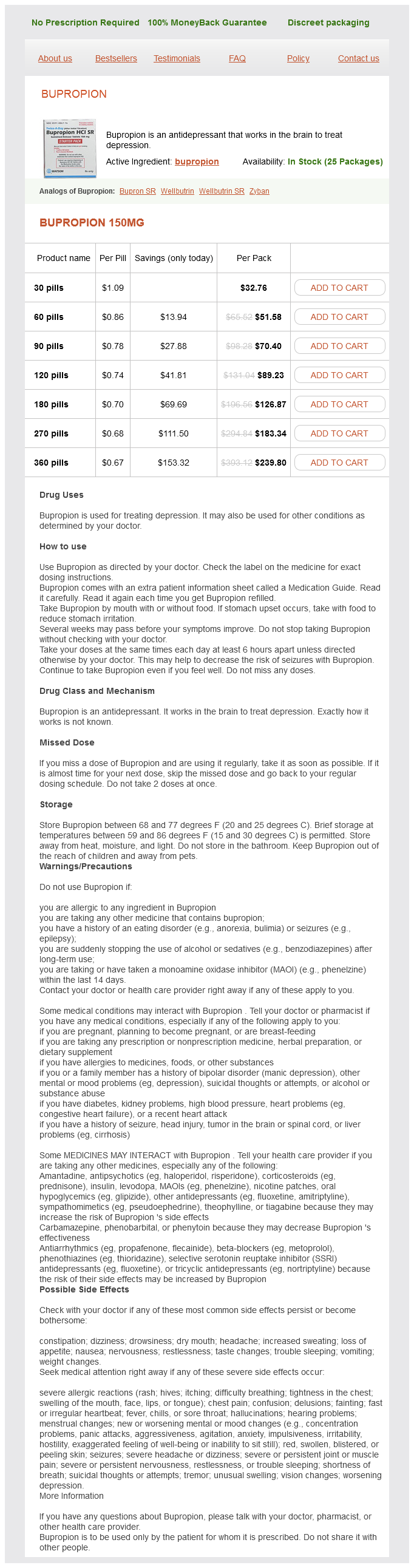
Bupropion dosages: 150 mg
Bupropion packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Only $0.71 per item
In stock: 527
Description
When the pressurizer is removed from the femur anxiety uncontrollable shaking cheap 150 mg bupropion overnight delivery, the void created should be filled with more cement. The surface of the cement is then dried with a sponge, and cement is used to coat the femoral stem, concentrating on the metaphyseal region. Both of these measures are intended to diminish the amount of blood, fluid, and other debris present in the cement and at the cementprosthesis interface. If the femur has a relatively wide diaphysis, the addition of a distal centralizer to the stem is advised to reduce the risk of varus malpositioning. Pre-heating the stem will further reduce cement porosity and accelerate cement polymerization. Insertion is started by hand, impacting the insertion device with a mallet as needed. Once the position of the trial stem has been reproduced, gentle pressure is maintained on the stem while excess cement is removed, and cement around the stem is pressurized by finger pressure. Once the appropriate head is selected, the trunion of the stem is carefully cleaned and dried, and the implant is gently impacted in place. The acetabulum is cleared of debris using irrigation and suction, and reduction is performed. The quadratus femoris is repaired to its insertion using nonabsorbable suture, along with repair of the gluteus maximus insertion if this tendon was released. A figure-8 suture is placed approximating the superior aspect of the piriformis to the abductor musculature; this suture is not tied initially. Repair of the short external rotators and posterior capsule to the posteromedial aspect of the greater trochanter is facilitated by two steps performed earlier in the case. These sutures typically are placed after acetabular cementing and before femoral preparation. During closure, the two sutures are passed through drill holes in the greater trochanter and tied to each other. To reduce operating time, the drill holes are created while waiting for the femoral cement to dry. Prior to tying the sutures, the leg is abducted and externally rotated, taking tension off the posterior soft tissue flap being repaired to the greater trochanter. The repair should be inspected carefully to make sure that the posterior flap is in contact with the femur, rather than hanging by suture or sutures, before the fascia is closed. The wound is once again copiously irrigated and routine closure of the fascia, subcutaneous tissue, and skin is performed. Patients with particularly high offset should be warned that mild lengthening of the leg may be necessary to achieve appropriate soft tissue tension. However, small skin incisions that limit exposure may place important deeper structures at risk for increased trauma. Optimal cement fixation of the acetabular component is difficult to achieve without a dry surgical field, making hypotensive anesthesia a crucial aspect of cement technique. Preoperative recombinant human erythropoietin may be considered in patients unable to donate blood.
Syndromes
- Brain damage
- Low blood pressure when getting up, sweating, drooling, lack of body temperature control. These problems are due to something called autonomic dysfunction.
- Problems swallowing
- Injury of the kidney and ureter
- Difficulty falling asleep
- Hepatorenal syndrome
- Use sunscreen. Sun protection with broad spectrum sunblock that works against UVA rays is important.
- Abdominal pain due to pancreatitis (inflammation of the pancreas)
- Blood chemistry tests (such as albumin level)
- Amyloid
In knees without deformity mood disorder in spanish 150 mg bupropion order, external rotation usually results in removal of more bone from the medial posterior condyle. Erosion of the posterior femoral condyles can distort this posterior condylar axis. To obtain an exact measurement of the patellar thickness, the prepatellar bursa should be dissected to completely expose the anterior surface of the patella. Femoral component rotation is determined by reference lines used for performing the distal femoral cut. An osteotome is used to free small remnant portions of uncut bone and removing posterior osteophytes. Calipers are used to assess the patellar thickness before the retropatellar osteotomy. In knees with complex or severe deformity, however, cautious stepwise release is necessary. Insert the trial components and check the balance of the knee after each step of the procedure. When the deformity is severe and leads to loss of the integrity of the ligaments, be ready for application of a constrained prosthesis. To achieve a proper soft tissue balance, initially remove the offending osteophytes until the anatomic margins of the bone are determined. Correction of Valgus Deformity Correction of Flexion Contracture Use a curved osteotome to release osteophytes in the back of the femur and then extract them with a rongeur. Strip the adherent capsule from the posterior aspect of the femur to reestablish the original recess. In knees with preoperative moderate to severe flexion contracture, it also is necessary to cut the posterior capsule transversely and to release the tendinous origins of the gastrocnemius. Correction of Valgus Knee With Incompetent Medial Collateral Ligament Correction of Varus Deformity the medial capsulotomy, along with subperiosteal medial release, which is included in the initial approach and exposure, can correct minimal varus deformities. A valgus knee with an incompetent medial collateral ligament occurs in knees with severe, longstanding valgus deformity. Next, insert a tibial sizing tray that matches the surface area of the tibial cut. This sizing tray is a jig for drilling final fixation holes for the tibial component and determines its ultimate mediolateral, anteroposterior, and rotational position. Check all around the tray to ensure that there is no overhang, especially on the medial side, where overhang may be easily overlooked. Apply varus and valgus stresses in both flexion and extension to determine the stability of the knee and the appropriate thickness of the tibial insert. Impact the stemmed tibial trial to ensure proper fit before implanting the final prosthesis. Drill the tibial plateau in the sclerotic parts (1 to 2 mm deep) to achieve adequate anchorage of the tibial component.
Specifications/Details
Sakau (Kava). Bupropion.
- Are there safety concerns?
- Is Kava effective?
- How does Kava work?
- What other names is Kava known by?
- Reducing withdrawal symptoms in people who need to stop taking anti-anxiety and sleep medicines called benzodiazepines.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96842
The patient may return to normal daily activities as tolerated 4 weeks after surgery and may return to contact sports or running 6 months after surgery depression symptoms and warning signs discount 150 mg bupropion with amex. Analysis of our first 23 consecutive cases demonstrated good or excellent clinical results in 22 of the 23 hips at a mean 18 months of follow-up. Historically, patient selection, surgical technique, and component designs have been less than ideal. In the normal knee, most of the ligaments are at their resting, unstretched lengths in extension. At 90 degrees of flexion, the lateral compartment will distract 7 mm while the medial compartment maintains a constant 2-mm gap. In a single-leg stance, the load across the medial compartment is approximately 70%. Unlike tricompartmental disease, unicompartmental disease should not require any ligamentous release during arthroplasty. Each additional millimeter of bone lost will result in increasing varus deformity of 1 degree. Varus deformity also will be maintained in flexion as the posterior cartilage is worn. Pain usually is recognized along the medial joint line, but its localization is unreliable. Pain is felt on standing and walking but usually is absent with sitting or lying down. The deformity corrects with 90 degrees of flexion and upon valgus stress at 20 degrees of flexion. Flexion contracture often is present, as are a joint effusion and synovial swelling. Cartilage and bone erosions are found on the anteromedial tibial plateau and distal surface of the femur, representing a pattern of extension disease. Erosions rarely extend to the posterior quarter and never to the posterior joint margin of the tibial plateau. The intact ligaments maintain normal femoral "rollback," resulting in this typical pattern of wear. However, when the capsule is relaxed at 20 degrees of flexion, the knee can be corrected manually to its prediseased alignment. At 90 degrees of flexion, the knee corrects spontaneously as the cartilage on the flexion surface of the femur comes in contact with the posterior tibia. A valgus stress view radiograph demonstrates realignment of the ligaments and preservation of the joint space. This will demonstrate the normal thickness of the cartilage in the lateral compartment and show whether the varus deformity is correctable. The lateral compartment should not measure less than 5 mm (the sum of the thickness of the normal cartilage), and the medial compartment should gap at least 5 mm (the sum of the articular cartilage lost).
Related Products
Additional information:
Usage: q.d.
Tags: buy bupropion 150 mg on-line, bupropion 150 mg buy low price, bupropion 150 mg order otc, bupropion 150 mg order on line
10 of 10
Votes: 200 votes
Total customer reviews: 200
Testimonials
Kerth, 23 years: Supplemental allograft mixed with highly concentrated platelet aspirate is then placed within the involved joint spaces. Furthermore, 70% of patients with advanced, terminal carcinoma demonstrate bone metastases at autopsy. When it is between two sizes, select the smaller size because mild notching (not more than 12 mm) is more palatable than overstuffing the patellofemoral joint. Line drawn parallel to superior border of S1 unreliable because of the rounding of the superior sacrum occurring secondary to the slip.
Esiel, 64 years: My preference in such situations is for bone transport-either double or single level-in which the overall length of the limb is maintained and the large bone gap at the knee is filled with the transported bone. Treatment of femoro-acetabular impingement: preliminary results of labral refixation. Guidewires can be inserted at the most cephalad portion of the osteotomy, directed toward the inner wall just above the triradiate cartilage. In this patient, a femoral shortening osteotomy and open reduction have been performed and sutures are in place allowing for a capsulorrhaphy once Pemberton osteotomy has been completed.
Giacomo, 37 years: Decreasing the overall thickness of the patella can result in extensor mechanism weakness. The patient must have been prepared in advance for a possible conversion to a total knee arthroplasty if not all the criteria are met. Approach the preferred surgical approach is a standard medial parapatellar approach, although an extensile approach may be necessary (see Chaps. The same operative technique can be used for correction of the proximal femur in abduction, flexion and extension, and rotation, and every combination thereof.
Hatlod, 58 years: No genetic defect has been identified, and no common teratogen is linked to fibular deficiency. This child had undergone a closed reduction and adductor tenotomy at 12 months of age. In the region of the peroneal tendon sheath attachment, the tendons are retracted anteriorly and the dissection is continued on the deep layer, above the abductor fascia. Through bending, these narrow-gauge staples have afforded dramatic correction of fixed knee flexion deformity.
Knut, 55 years: It may be advisable to place a cable at the level of the sleeve at this point to prevent fracture. Ideally, the pin should be separated from the other pins maximally at the fracture site. The shaft is supplied by a single nutrient artery that enters from the medial cortex at the junction of the proximal and middle thirds of the diaphysis. Examination under anesthesia for femoral anteversion and coronal-plane malalignment of the knee should be accomplished before positioning.
Goran, 49 years: The first radiographic signs of new bone formation indicate the reossification stage. We use a single dose of warfarin preoperatively on the day of surgery, a single dose of intravenous heparin given intraoperatively prior to hip dislocation, and adjusted-dose warfarin postoperatively for the first 2 to 3 days in all patients. Functional results after revision of well-fixed components for stiffness after primary total knee arthroplasty. The fourth and fifth tarsometatarsal (lateral column) joints have distinctly more inherent motion and are critical in accommodation of the foot to uneven surfaces.